Let's take a quick look at the "CD4 Count" procedures described by the US Centers for Disease Control (CDC) and the World Health Organization (WHO).
These procedures claim to count how many CD4+ T Lymphocytes ("CD4") are in one cubic millimeter of blood. This cell type, the so-called CD4 cells, is claimed to be the target of so-called HIV.
It is claimed, but was never proven, that HIV infects and kills CD4 cells. In the US, a CD4 count below 200 is sufficient for a diagnosis of AIDS for someone who has tested HIV+. A diagnosis of AIDS is usually accompanied by a prescription for so-called "Anti-Retro-Viral ARV drugs.
CD4 counts are also used to draw conclusions about how well ARVs are working. Are those conclusions valid? We're going to find out shortly, but consider this: If you gave me a count, I could not tell you if it came from someone who tested antibody positive or negative. However, the reaction by the medical profession is quite different. If you are so-called HIV+ and have a count below 400, they often recommend drugs. In the US, if the count is below 200, they diagnose the person as having AIDS --but only if the person is also tested "HIV+." In fact, even though people who test negative can have very low CD4+ counts, apparently it's not important. In fact, only those diagnosed as HIV+ are even subjected to the CD4+ count procedures. Double standard? You bet. Scientific? Not.
The goal here is to look at the procedure, and see what is happening. Then we'll look at the research.
Please open the links provided and read them along with what is written here.
A. "TriCount Method" for counting CD4 cells -- the U.S. Centers For Disease Control (CDC)
http://www.cdc.gov/mmwr/PDF/rr/rr4602.pdf
We see that they end up with a "count" [except that it is not a count] of number of CD4 cells per cubic mm (aka CD4+ T helper cells or CD4+ T lymphocytes).
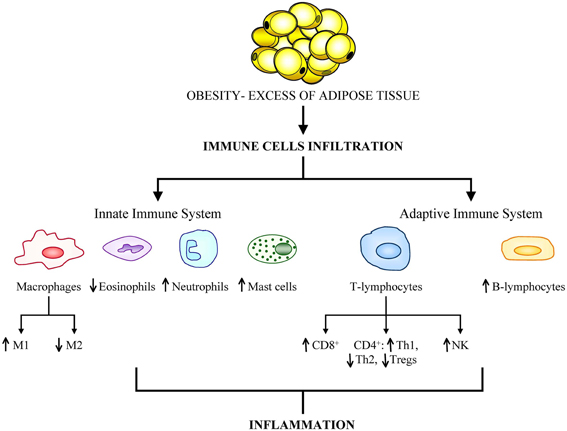
Note that this is as far as they go. They easily could develop a test to measure the subtypes of CD4+ T cells -- but they don't. Remember those subtypes from the previous post? Th1, Th2, Th17, etc. Let's go back and look at the diagram:
This test does not count these subtypes. Neither do the procedures described by WHO. Is it important? The research that we will look at later suggests that it is very important to know the counts of the subtypes, and we will learn why. Not knowing them may lead to false conclusions, including false conclusions about exactly how the ARVs are affecting the CD4+ counts, according to research that we will examine later.
For now, just note what's happening here with this procedure. No Th1, no Th2 -- no subtypes of CD4+ T helper cells. And counts that are not counts and that may be highly inaccurate.
Reading this also provides a glimpse of the setting in which this magic counting is taking place. Flipping through the pages, you can see that this is an elaborate procedure requiring sophisticated lab instruments and lab personnel with high technical skills. At the same time the people doing this have to take all kinds of safety precautions because they are warned to be afraid of catching AIDS or other diseases from handling human blood. Those are their working conditions. Can you imagine the results that may emerge under such conditions?
We are not lab techs, but I posted this so we can get a feel for what's going on, and focus on the important points.
Can you imagine the stress of doing this kind of work day after day? Safety, precise measurements, everything has to be done with the greatest care. Handling blood, numerous reagents, laboratory instruments, etc. This is stressful work. So you have to hope you get someone who is well qualified, super conscientious and focused, and not having a bad day. This is the lab technician's work, day after day. It is more challenging than other lab tech work. We should believe that these are super human beings. But they're not, and so we shouldn't.
On pages 7 - 8 we see that the CD4+ T cells are not really "counted." They are "calculated" to give an "estimate." An instrument is used, along with chemicals that absorb and emit light, and the percentage of cells that is CD4+ is calculated. From that an absolute number of cells is calculated.
On page 8, look at: "8. Reportable Range." Here they tell you about other cell types, which we've seen in the last posting, and how they are distinguished, and that's the last we hear of them. But there is no mention of the subtypes of CD4+, which are the cells of interest. Why bother with these other cells and not nail down the breakdown of specific subtypes of the CD4?
Let's keep reading. Look at all the steps -- and all the things that can go wrong. Flipping to p. 9 we see troubleshooting tips.
Finally, if everything goes right, we have a CD4+ "count" (that is actually a calculated estimate) and that is a lump sum of all of the subtypes. We don't know the breakdown.
This is as good as it gets. When we look at the WHO procedures, we'll see even more problems.
The thing is, when your doctor orders this test, does he or she tell you what procedure is used or how this is actually done? If you have had this test, start asking questions. Which procedure was used to test your blood? Can you get a tour of the lab? Can you meet the team who tested your blood? Why not? This is just as important as meeting your doctor. Why? Because their results can affect your life.
As we will see, a CD4 "count" easily could be very inaccurate, that is, "way off." It's not the lab tech's fault. So many things can go wrong, and they have a lot of work to do. This is only one of many procedures. The choice of procedures can be a major factor as well, in determining what the CD4 "count" is and how accurate it is.
Even if you are lucky enough to get an "accurate" CD4+ estimate, will it be properly interpreted? Or will conclusions be drawn that are wrong?
Regardless, we will not get the "counts" for the CD4+ subtypes with any of the procedures described by the CDC or the WHO. That is a very serious shortcoming of all of these procedures.
B . "Laboratory Guidelines for enumerating CD4 T Lymphocytes in the context of HIV/AIDS" --World Health Organization (WHO)
The World Health Organization (WHO) has published a 68-page guide entitled "Laboratory Guidelines for enumerating CD4 T Lymphocytes in the context of HIV/AIDS."
The title alone should raise a red flag. Why does counting CD4 T Lymphocytes need to be considered "in the context of HIV/AIDS?" "HIV/AIDS" should not be a factor in "counting" T cells.
But we know that it is! Because, to the medical profession working for the HIV/AIDS Industry, a low CD4 count means nothing unless you tested HIV+. If you are HIV-, your CD4+ count is so un-important that it is not even measured! Imagine that.
The publication lists many different methods or "counting" CD4 cells, from microscope examination to various methods using flow cytometry technology, like the one described by the CDC. Again, we are talking about calculated estimates, not counts, and they can be way off because small errors get multiplied and therefore magnified.
They also include HIV/AIDS/ARV info that has nothing to do with the CD4 "counting" procedures, per se, but have to do with interpretation in the context of HIV/AIDS. For example, on page 14, this statement appears: "In response to successful ART, the CD4 T lymphocyte count typically increases by >50 cells/µL within weeks after viral suppression, and then increases 50-100 cells/µL per year thereafter until a threshold is reached. In some patients, CD4 T lymphocyte counts may not increase as quickly or as steadily, even with durable viral load suppression. "
In other words, even when what they call "viral load" drops and stays low, the CD4s do not always go up. Maybe the viral load isn't a viral load? Maybe the "virus" is not the culprit after all? There could be many reasons, and they don't offer any, but never once do they consider that their premise could be false. Maybe HIV has nothing to do with what they're looking at. We'll be analyzing all of this shortly.
WHO lists a number of methods and "alternate methods" for "counting" CD4 cells, and the pros and cons of each. Some methods, like counting under a microscope, actually do involve counting cells. But too few cells are counted and then the number counted is multiplied to get the estimated result. That's how a small error gets multiplied into a big error.
With flow cytometry, antibodies with fluorescent tags are reacted with blood cells and attach to the CD4 protein. The fluorescence from the attached tagged antibodies is measured, and, after a series of calculations laden with assumptions that may or may not be accurate, a "count" results. It is in reality a very rough "estimate" (NOT a "count") that may well be based on false assumptions and is almost impossible to duplicate if you take the same sample of blood and run it again in the same lab! Do the procedure in another lab, and the estimate will likely be even more different. Use a different procedure in a different lab, and ... well, you get the picture.
To appreciate how arbitrary and imprecise the whole "CD4 count" testing system is, take a look at page 32, which tells you what standards to use in selecting the right method:
"4.3 Selections of methodology for CD4 T lymphocytes count estimation. For efficient and optimum reporting of CD4 counts, the proper selection of the methodology is essential (Table 4.1).
The choice of the assay should depend on:
Purpose of the assay (whether it is being used for monitoring or for research
p. 33 The age group of the patients (whether adult or pediatric: to indicate whether CD4 percentages or absolute counts are required)
Sample turnover (no. of samples to be tested/day)
Availability of stabilized electric power supply and space
Location of testing (whether rural or urban and whether at primary health centre, district or central referral centre)
Availability of technically skilled personnel as required (the current methods require varying degrees of technical skills)
Availability of technical support and equipment (regular maintenance is necessary)
COST: The cost should include instrument and reagent cost as well as hidden cost of labour (often less expensive), disposables (if available often more expensive), shipping costs, infrastructure, repeat assay run and instrument repair
The time within which the assay can be performed from the time of blood collection.
Technologies that have not been adequately validated should not be purchased."
What else could go wrong?
The staff "should be" qualified, well trained and have continuing education.
The accuracy of CD4 testing results depends on the quality of the blood sample submitted to the laboratory.
" ..the laboratory director or manager should review the results of testing before reporting the results."
"To obtain an accurate and precise enumeration of absolute CD4+ T cells, an accurate measurement of blood is required."
What does this imply?
If the procedures are repeated in the same lab, different labs and using different procedures as well, if the results are close, then and only then should you be confident that the "counts" are accurate.
But even if you do all of that, you still don't have the CD4 T Lymphocyte sub types (Th1, Th2, etc.) AND you still don't have a medical profession that will correctly interpret the results. Most of them are unaware of the research, and that's what we'll be looking at next.

.gif){kind=link}
{kind=link}